
Vaccines
Canine Factsheet
Two vaccines which were initially commercialized are not available anymore. The first one was launched in Brazil and was based on a fucose-mannose ligand enriched with glycoprotein 63 with a saponin adjuvant and the second one, the first launched in Europe, was based on purified excreted/secreted antigens of L. infantum combined to a saponinlike adjuvant.
The only currently available vaccine in Europe contains the active substance “protein Q”, a recombinant protein containing five different antigens from L. infantum without an additional adjuvant. First vaccination is a single injection. Booster injections are given annually.
The vaccine available in Europe can only be injected to healthy seronegative dogs, 6 months of age or older, tested by a quantitative serological assay.
A new DNA vaccine based on the non-replicative antibiotic resistance marker-free plasmid vector pPAL which contains an encoding gene for the L. infantum activated protein kinase C receptor analogue (LACK) has been approved by the European Medicines Agency in 2023. This vaccine can only be administered via intranasal, to healthy dogs of 6 months of age or older.
All of these vaccines do not prevent infection but do alter disease progression and the probability of progression to clinically overt disease.
Table 7. Current anti-Leishmania vaccines for dogs
| Commercial name (manufacturer) | Composition | Availability | Vaccine protocol | Primary outcome | Vaccine efficacy | Diagnostic interference associated with vaccine | |
| Antigen | Adjuvant | ||||||
| Leish-Tec® (Ceva Santé Animale)* | A2 | Saponin | Brazil | Three primary vaccination doses (SC), 21-day intervals; one annual booster | Parasite detection | 71.4% | Yes |
| Letifend® (Leti Pharma laboratories) | Q-protein | None | Europe | One primary vaccination dose (SC); one annual booster | Clinical disease | 72% | No |
| Neoleish® (CZ Vaccines S.A.U.) | DNA plasmid containing LACK gene | None | Spain | One primary vaccination dose (intranasal); one booster every 6 months | Clinical disease | - | No |
* Currently not available.

Prevention
Canine Factsheet
Prevention for individual dogs (healthy, infected clinically healthy and sick) should always include use of a topical insecticide with proven efficacy maintained throughout the period of sand flies activity. Additionally, vaccination should be considered as a part of a multimodal approach*.
Only insecticides that have been approved by the formal approval body should be used for the prevention of CanL.
Topical insecticides applied to dogs living in or travelling to endemic areas should be maintained during the entire period of potential exposure to sand flies:
A. Spot on formulations
Treatment with permethrin spot-on formulations may provide a repellent (anti-feeding) activity against sand flies for 3-4 weeks. In the case of dogs travelling to endemic areas, the product should be applied at least 2 days before exposure.
B. Collars
Collars impregnated with deltamethrin prevent phlebotomine sand fly bites for varying periods depending on the manufacturer, even up to 12 months for one of the products.
A flumethrin in combination with imidacloprid-containing collar, with proven repellent efficacy against sand flies, has shown in clinical field studies a reduction of the risk of infection with L. infantum transmitted by sand flies for up to 8 months.
All the collars should be applied at least 1-2 weeks before exposure.
*Based on a risk-benefit assessment from endemic areas, a multimodal approach combining repellent use and vaccination should be considered for optimal prevention of both infection and development of clinical disease. Repellents highly reduce the risk of infection but do not prevent the appearance of clinical signs once the dog has been infected. Vaccination reduces the risk that infection would progress to disease and the probability of clinical signs developing, but it does not prevent infection.
Table 6. Preventative recommendations based on different level of risk for L. infantum infection
| NON ENDEMIC AREAS | ||||
| Level of risk (0 low - 4) | Travel history | Lifestyle | Preventative applications | Additional recommendations |
| 0 | Local (negligible) | Any | None | Avoid breeding with or blood transfusion from dogs belonging to risk levels 3-4 and any PCR positive or seropositive dogs (and 1-2, if possible) |
| 1 | Occasional travel to fringe or endemic areas | Any | Repellents: Cover the entire period of travelling /exposure including the delay for activity | See risk level 0 If travel once for less than 3 weeks, use topical insecticide spot-on formulations applied at least 2 days before exposure. For longer periods of travel, use repeated spot-on or collars. Test for L. infantum infection 6 months after travel (by quantitative serology only) |
| 2 | Frequent/long travel to fringe or endemic areas | Any | Repellents: Cover the period of travel including the delay for repellent activity. Vaccination (optional) | See risk level 0 For long and/or frequent trips preventative and additional recommendations should be the same as for risk level 4. Test for L. infantum infection 6 months after last exposure (by quantitative serology). Domperidone/Nucleotides + AHCC could be considered (if not vaccinated) |
| 3 | Re-homing from an endemic area | Any | See additional recommendations | Test for L. infantum infection via quantitative serology. If positive, do not breed and do not use as blood donor, consider treatment (see staging). Repellents all year round Testing of other household dogs |
| ENDEMIC AREAS | ||||
| Serology Results (IFAT/ELISA) | Lifestyle | Preventative applications | Additional recommendations | |
| 4 | Seronegative | Outdoors (high exposure) | Repellents all year round or during the known sand fly transmission season. Vaccination (strongly recommended) | Domperidone/Nucleotides + AHCC could be considered (if not vaccinated). Periodic testing (by quantitative serology) if breeding or blood donor (at least once a year) |
| Indoors (low exposure) | Repellents all year round or during the known sand fly transmission season. Vaccination (optional) | Domperidone/Nucleotides + AHCC could be considered (if not vaccinated). Periodic testing if breeding or blood donor Domperidone could be considered (if not vaccinated) | ||
| Non applicable | Seropositive (Healthy*/Sick**) | Any | Repellents all year round | Do not use for breeding or as blood donor Staging for treatment as needed Test other household dogs |
ELISA: Enzyme-linked immunosorbent assay – IFAT: Indirect Fluorescent Antibody Technique
*Healthy: a dog without any clinical sign or clinicopathological abnormality
**Sick: a dog with clinical signs and/or clinicopathological abnormalities attributed to Leishmania
Monitoring
Canine Factsheet
Table 5. Recommended monitoring during and after treatment of CanL
| Parameters | Frequency | |
|---|---|---|
| Clinical history and physical examination CBC, biochemical profile ± serum electrophoresis Complete urinalysis ±UPC | Sick treated dogs | Clinically healthy infected dogs |
| After the first month of treatment and then every 3-4 months during the first year. Thereafter, every 6-12 months in dogs fully recovered clinically with treatment. | Every 3-6 months(see figure 2) | |
| Quantitative serology* | Not before 3 months after initial treatment and every 6-12 months. | |
| Real-time PCR (optional)** | At the same time as serology. | |
* Some dogs have a decrease in antibody levels (i.e. on IFAT results at least a 2-3 fold dilutions difference between monitoring samples) associated with clinical improvement within 6-12 months of therapy. An increase in antibody levels (i.e. at least 2-3 fold dilutions difference between monitoring samples) should be interpreted as a marker of disease relapse, especially following the discontinuation of treatment.
** Sensitivity of PCR assays relies considerably on the type and number of tissues evaluated. Bone marrow, lymph node, spleen, and cutaneous lesions are better targets for Leishmania detection than whole blood. Testing two to three samples of different tissues are recommended for a more accurate diagnosis.
Figure 2. Recommended monitoring during and after treatment of CanL
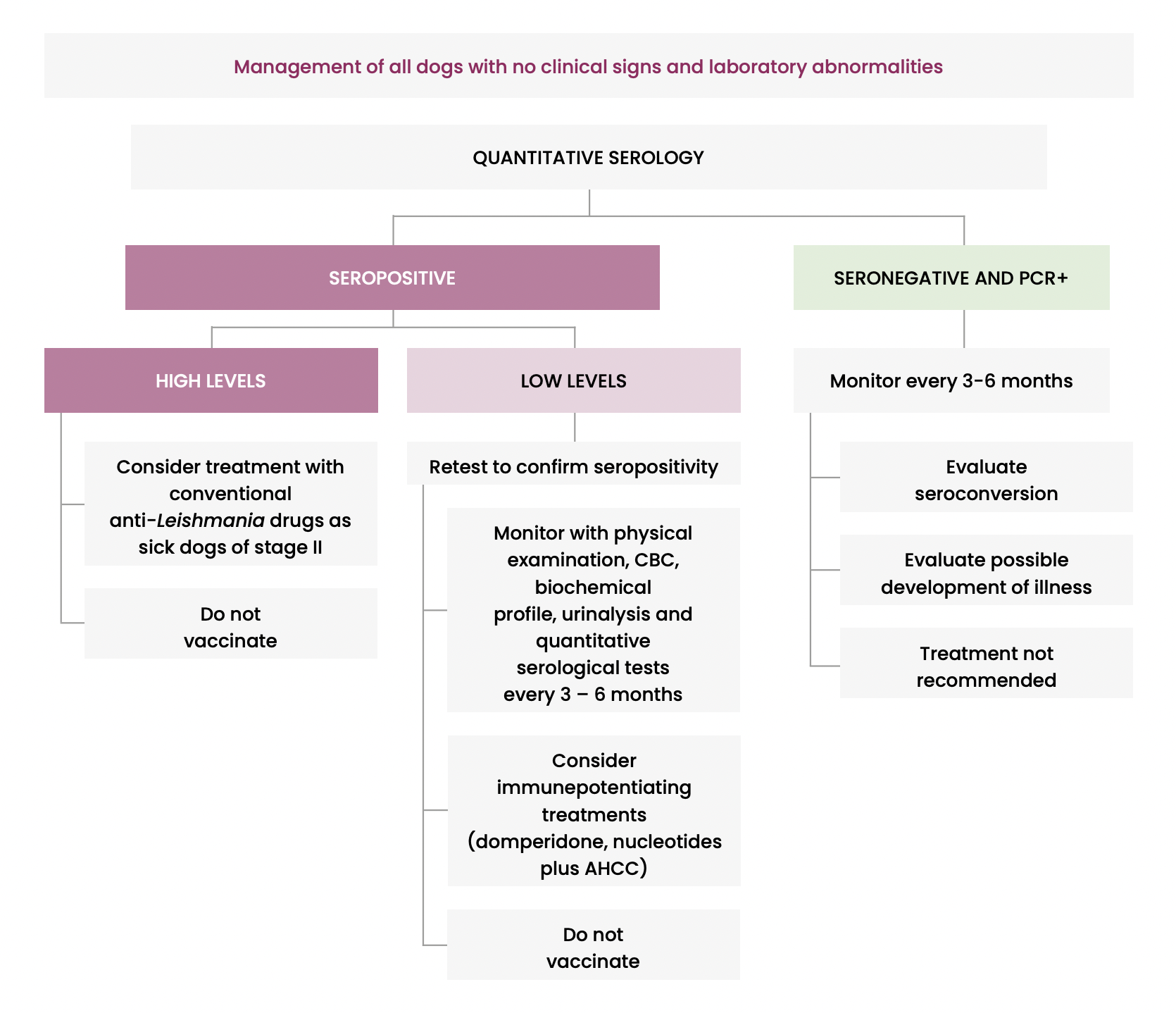
It is recommended to use serology alone or the combination of serology with PCR for screening healthy dogs and to avoid screening clinically healthy dogs (not vaccinated) only by PCR.

Therapy
Canine Factsheet
Table 4. Current treatment protocols for CanL
| Drugs | Dose | Main side effects |
| Meglumine antimoniate A | 100 mg/kg SC*, once a day or divided in two doses, for 4-6 weeks (initial reduced dosages for 2-3 days may be useful to detect any adverse events) B | Potential nephrotoxicity Pain and inflammation at injection site |
| Miltefosine A | 2-2.5 mg/kg PO, once a day for 28 days** | Disorexia Vomiting Diarrhea |
| Allopurinol | 10mg/kg PO, twice a day for 6-12 months (depending on the staging and the side effects***) | Xanthine urolithiasis Renal mineralization Nephrolithiasis |
| Domperidone C | 0.5 mg/kg PO, once a day for 1 month and following manufacturer instructions | Galactorrhea |
| Dietary nucleotides with AHCC C-D | Once a day, PO. Following manufacturer instructions, for 6-12 months |
A Registered for veterinary use in most European countries; both therapies are recommended in combination with allopurinol.
B There is a limited number of studies on optimal treatment regimen.
Recommended dosages off-label but according to pharmacokinetic and clinical studies in dogs. Treatment may be extended by 2-3 weeks in patients stages II and III (without CKD) and with severe clinical picture or laboratory abnormalities.
C To be considered as monotherapy only for stage I.
D To be considered, as an alternative to allopurinol, in dogs with xanthinuria due to allopurinol side effects.
AHCC: Active hexose correlated compound – PO: Per os – SC: Subcutaneous
* Injections should be administered in different skin sites.
** To reduce side effect administered always with food.
*** Monitoring side effects with urinalysis and abdominal ultrasound is recommended periodically.
Disclaimer: Information given here on drugs and dosages are based on a consensus of clinical and scientific experience by the LeishVet members. Most recommendations have been published in scientific peer-reviewed journals. Veterinary practitioners are requested to check with product leaflets and product registrations in their related country prior to any product selection and initiation of treatment.

Clinical Staging, Treatment and Prognosis
Canine Factsheet
Table 3. Clinical staging in CanL
Staging is performed following canine patient diagnosis of L. infantum infection with clinical signs and/or clinicopathologic abnormalities to facilitate appropriate treatment and monitoring of the patient). Infected but clinically healthy dogs are not included in this staging (see below).
| CLINICAL SIGNS | LABORATORY FINDINGS* | QUANTITATIVE SEROLOGY** | SPECIFIC THERAPY | PROGNOSIS | |
| STAGE I Mild disease | Mild clinical signs such as example papular dermatitis or localized lymphadenomegaly | No clinicopathological abnormalities observed. Normal renal profile: creatinine < 1.4 mg/dL, non-proteinuric: UPC< 0.5 | Negative to low positive antibody levels. | Scientific neglected*** | Usually good |
| STAGE II Moderate disease | Diffuse or symmetrical cutaneous and/or mucocutaneous lesions such as example exfoliative, ulcerative or nodular dermatitis, onychogryphosis, generalized lymphadenomegaly, loss of appetite and weight loss. | Clinicopathological abnormalities compatible with L. infantum infection such as example mild non-regenerative anemia, hypergammaglobulinemia and hypoalbuminemia. Substage a) Normal renal profile: Creatinine < 1.4 mg/dl; non-proteinuric: UPC < 0.5 b) Creatinine < 1.4 mg/dL; proteinuric (UPC= 0.5-1) | Low to high positive antibody levels. | Meglumine antimoniate + allopurinol Miltefosine + allopurinol Substage b: Follow IRIS Guidelines (†) for CKD | Good to guarded |
| STAGE III Severe disease | Dogs, which apart from the signs listed in stages I and II, may present signs originating due to immune-complex deposition (e.g. glomerulonephritis, uveitis). | Clinicopathological abnormalities listed in Stage II. CKD IRIS stage 1 with proteinuria UPC > 1 or CKD IRIS stage 2 (creatinine 1.4-2.8 mg/dl) | Usually high positive antibody levels. | Meglumine antimoniate + allopurinol Miltefosine + allopurinol Follow IRIS Guidelines (†) for CKD | Guarded to poor |
| STAGE IV Very severe disease | Dogs with clinical signs listed in Stage III. Pulmonary thromboembolism, or nephrotic syndrome and end stage renal disease. | Clinicopathological abnormalities listed in stages II and III. CKD IRIS stage 3 (creatinine 2.9-5 mg/dl) and CKD IRIS stage 4 (creatinine > 5 mg/dl) or nephrotic syndrome or marked proteinuria UPC > 5 | Usually high positive antibody levels. | Specific treatment should be instituted individually. Follow IRIS Guidelines (†) for CKD | Poor |
CKD: Chronic kidney disease – IRIS: International Renal Interest Society – UPC: Urinary protein:creatinine ratio
* Full CBC, biochemical profile with serum protein electrophoresis and urinalysis with UPC.
(†) IRIS recommendations must be strictly followed in stages III and IV (http://www.iris-kidney.com/)
** Infection should be confirmed via other diagnostic techniques such as cytology, histology/immunohistochemistry and PCR in dogs with negative to low positive antibody levels. High antibody levels, are conclusive of CanL.
*** Dogs in stage I (mild disease) are likely to require short treatment with one (meglumine antimoniate, miltefosine, allopurinol) or two conventional anti-Leishmania drugs (combination of meglumine antimoniate with allopurinol or miltefosine with allopurinol). Immune-potentiating treatments in conjunction with antileishmanial drugs or alone may be considered (domperidone, nucleotides plus AHCC). Alternatively, consider monitoring without treatment. There is limited evidence of treatment outcomes for dogs in this stage and, therefore, efficacy of these treatment options remains inconclusive.

Diagnosis
Canine Factsheet
Diagnosis is based on clinical signs and/or clinicopathological abnormalities compatible with disease combined with demonstration of L. infantum infection, by using serological and/or molecular techniques. However, cytology and histology combined with immunohistochemistry can be used to directly correlate Leishmania infection with the disease.
Main purposes for the diagnosis of L. infantum infection:
A. Confirm the disease in a dog with clinical signs and/or clinicopathological abnormalities compatible with leishmaniosis (Table 2 and Figure 1).
B. Screening of apparently healthy dogs living in or travelling from endemic areas:
- blood donors
- breeding dogs
- dogs prior to vaccination against CanL
- dogs admitted for the annual serological test for CanL
- imported dogs (from endemic areas)
Diagnostic approach
Figure 1. Flow chart for the diagnostic approach to dogs with suspected clinical signs and/or clinicopathological abnormalities compatible with leishmaniosis*
Clinical signs and/or clinicopathological abnormalities compatible with leishmaniosis
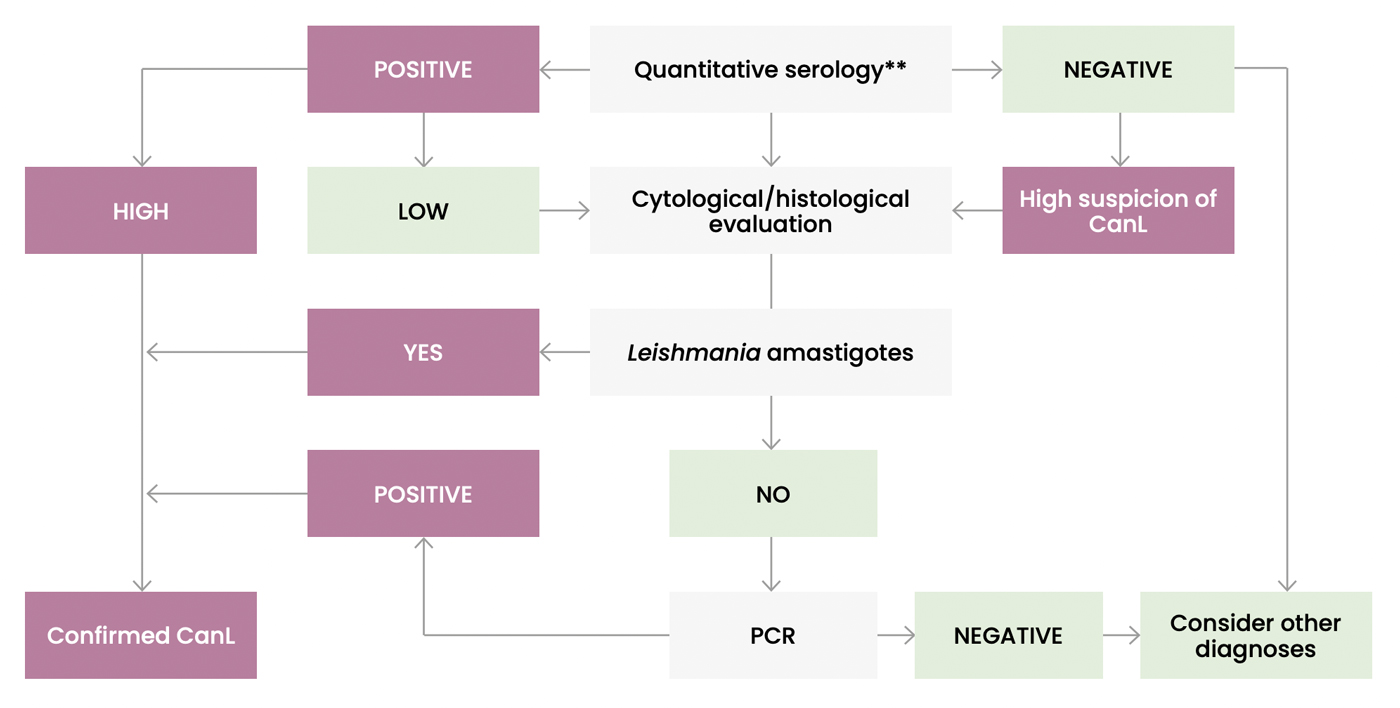
CanL: Canine leishmaniosis – PCR: Polymerase chain reaction
* This flow chart cannot be applied In case of recent vaccination against CanL with a vaccine known to induce cross reacting antibodies.
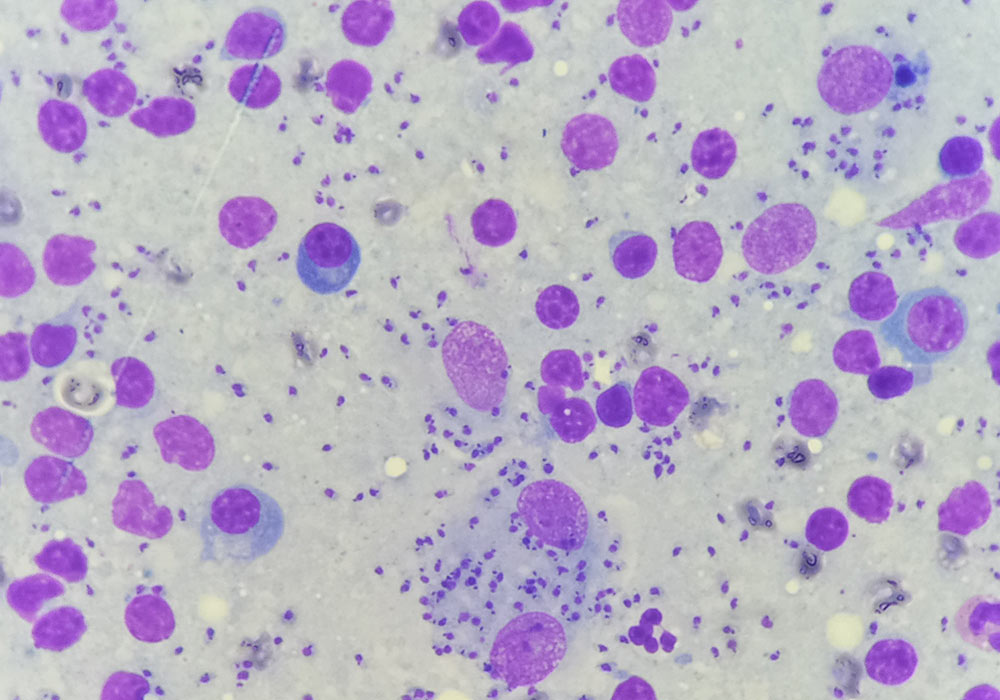
** Cytology could be performed at the same time in any damaged tissue or biological fluid.
Infected healthy versus infected sick dog
Dogs with clinical leishmaniosis are those presenting compatible clinical signs and/or clinicopathological abnormalities, and having a confirmed L. infantum infection. It should be emphasized that a dog may be sick due to another disease with similar clinical signs and simultaneously infected by L. infantum. Exclusion of other differential diagnoses is recommended in infected sick dogs.Dogs with subclinical infection (infected but clinically healthy) are those that do not present neither clinical signs on physical examination nor clinicopathological abnormalities on routine laboratory tests (CBC, biochemical profile and urinalysis) but have a confirmed L. infantum infection.
Diagnostic methods
Parasitological: cytology, histology/immunohistochemistry and culture.Molecular: conventional, nested and real-time polymerase chain reaction (PCR).
Serological: quantitative assays (IFAT and ELISA) and qualitative preliminary rapid tests.
What samples and techniques should be used for PCR?
Any lesional tissue or abnormal biological fluid compatible with L. infantum infection.Target organs: bone marrow, lymph node, spleen, skin.
Less invasive samples: conjunctival swabs.
The sensitivity of the PCR assay is much lower when performed on these samples: blood and urine.

Clinical Manifestations
Canine Factsheet
Table 2. Main clinical signs and clinicopathological abnormalities found in CanL due to L. infantum
MAIN CLINICAL SIGNSGeneralLocalized or generalized lymphadenomegalyLoss of body weight Decreased appetite Lethargy Pale mucous membranes Splenomegaly Polyuria and polydipsia Fever Vomiting Diarrhea CutaneousExfoliative dermatitis with or without alopeciaErosive-ulcerative dermatitis Nodular dermatitis Papular dermatitis Pustular dermatitis Nails abnormalities OcularBlepharitis (exfoliative, ulcerative or nodular) and conjunctivitis (nodular)Keratoconjunctivitis, either common or sicca Anterior uveitis Endophtalmitis OtherMucocutaneous and mucosal ulcerative or nodular lesions (oral, genital and nasal)Epistaxis Lameness (erosive or non-erosive polyarthritis, osteomyelitis and polymyositis) Atrophic masticatory myositis Vascular disorders (systemic vasculitis and arterial thromboembolism) Neurological disorders | CLINICOPATHOLOGICAL ABNORMALITIESCBC/HemostasisMild to moderate normocytic normochromic non-regenerative anemiaLeukocytosis or leukopenia: lymphopenia, neutrophilia, neutropenia Thrombocytopathy Thrombocytopenia Impaired secondary hemostasis and fibrinolysis Serum biochemical profile with proteins electrophoresisHyperproteinemiaHyperglobulinemia (polyclonal beta and/or gammaglobulinemia) Hypoalbuminemia Decreased albumin/globulin ratio Renal azotemia Elevated liver enzyme activities Proteinuria CBC: Complete blood count |










Etiology and Epidemiology (Distribution, Transmission)
Canine Factsheet
Leishmania infections in dogs are predominantly due to Leishmania infantum. However, other species of Leishmania may also infect dogs (most important species in dogs, their distribution and hosts are described in Table 1). Many species of Leishmania infect both humans and animals and are zoonotic.
The information in these guidelines is focused only on infection and disease due to L. infantum. This agent has a very wide distribution including the Mediterranean Basin, parts of Asia, and the Americas.
Leishmania spp. and more specifically L. infantum infection are typically transmitted by specific species of “insect vectors” belonging to the phlebotomine group (also called “sand flies”). These vectors represent the major route of transmission in endemic areas. The presence and activity of sand flies belonging to species competent for transmission defines the places where the infection or disease can be “endemic” in human and animal populations, including domestic dogs.
The vectors may transmit Leishmania infection to animals species other than human or dogs and a continuously increasing number and diversity of mammal species have been reported as infected including domestic (i.e. cat) or wildlife (i.e. rodents) both in rural and sylvatic environments or captive in zoos. At least some of these species are also active reservoirs with ability to be a source of infection for sand flies and consequently drive transmission of the infection to other receptive species. This results in a situation in which infected domestic dogs may represent, amongst others, a risk for human infection.
Non-vectorial transmission routes have also been demonstrated (sexual, vertical and blood transfusion). These modalities are far from being negligible and have been demonstrated in dogs. The non-vectorial transmission modalities may have a major impact in “non-endemic areas” where vectors are absent or present in very small numbers. In those areas, Leishmania infection may maintain mainly in and from stable foci. Non-vectorial transmission considerably extends the global distribution of the parasite and the potential concern for veterinary practitioners. As a consequence, the importation of infected animals from endemic areas may be the reason for the development of disease foci in non-endemic areas.
Table 1. The most significant species of Leishmania known to affect domestic dogs
| Species Genus | Distribution | Hosts | Zoonotic aspects |
| L. infantum | Mediterranean Basin, Middle East, South America (Brazil), parts of Asia (China, Central Asian Republics) Increasing in non-endemic countries (Europe, USA, South and Central America from Mexico to north Argentina) | Many groups of mammals found infected when looked: canids, felids, mustelids, rodents, rabbits and hares, bats, marsupials, humans, etc. | Visceral, cutaneous and mucocutaneous leishmaniosis |
| L. major | Southern Mediterranean Basin, Middle East, Arabic peninsula, central Asia to India, western/eastern Subsaharan Africa | Mostly wild rodents, occasional in carnivores, humans | Visceral, cutaneous and mucocutaneous leishmaniosis |
| L. tropica | North Africa, Balkan countries, Middle-East to central Asia, eastern Africa and Arabic peninsula | Humans (“anthroponotic”), rodents (hyrax in Middle East) | |
| L. braziliensis | Central and South America | Rodents, equidae, carnivores, humans | Cutaneous and mucocutaneous leishmaniosis |
Several other species have been detected in dogs with still limited information on their importance (L. amazonensis, L. mexicana, L. peruviana, L. panamensis). Concerning South American species, please visit Brasileish’s group website (www.brasileish.com.br).
Leishmania donovani infection in India and east Africa is typically anthroponotic (the disease is also called Kala Azar). The role of animals in L. donovani infection remains to be investigated.
Infection in the canine population in endemic areas is widespread, and the proportion of infected dogs is much higher than that of dogs with clinical leishmaniosis. Therefore, subclinical infection is common in endemic areas (clinically healthy infected dogs). Nevertheless, CanL is also often diagnosed in non-endemic countries (dogs imported from or travelling to endemic areas).
Susceptibility is related to the ability of the host to mount a protective specific immunity. A strong cellular immunity results in long term control of infection in resistant dogs. On the contrary, the development of an intense humoral response drives non-protective immunity which in return is largely responsible for clinicopathological disorders and clinical signs in susceptible dogs.